Alfie Cooper
Alfie Cooper A medical device can meet every clinical specification and still become a poor investment when technical support is slow, spare parts are unavailable, or warranty responsibilities remain unclear. Equipment downtime may delay diagnosis, interrupt procedures and force clinical teams to depend on backup systems or external providers.
For Healthcare buyers, those responsible for sourcing clinical equipment, service response should be evaluated before a purchase order is approved. Buyers need to know who will answer a fault report, how quickly the issue will be assessed and what resources are available to restore the equipment.
A stated warranty period does not answer these questions. Effective support depends on the engineer's availability, diagnostic capability, replacement parts, escalation procedures, and the supplier’s ability to work within the facility’s location and operating conditions.
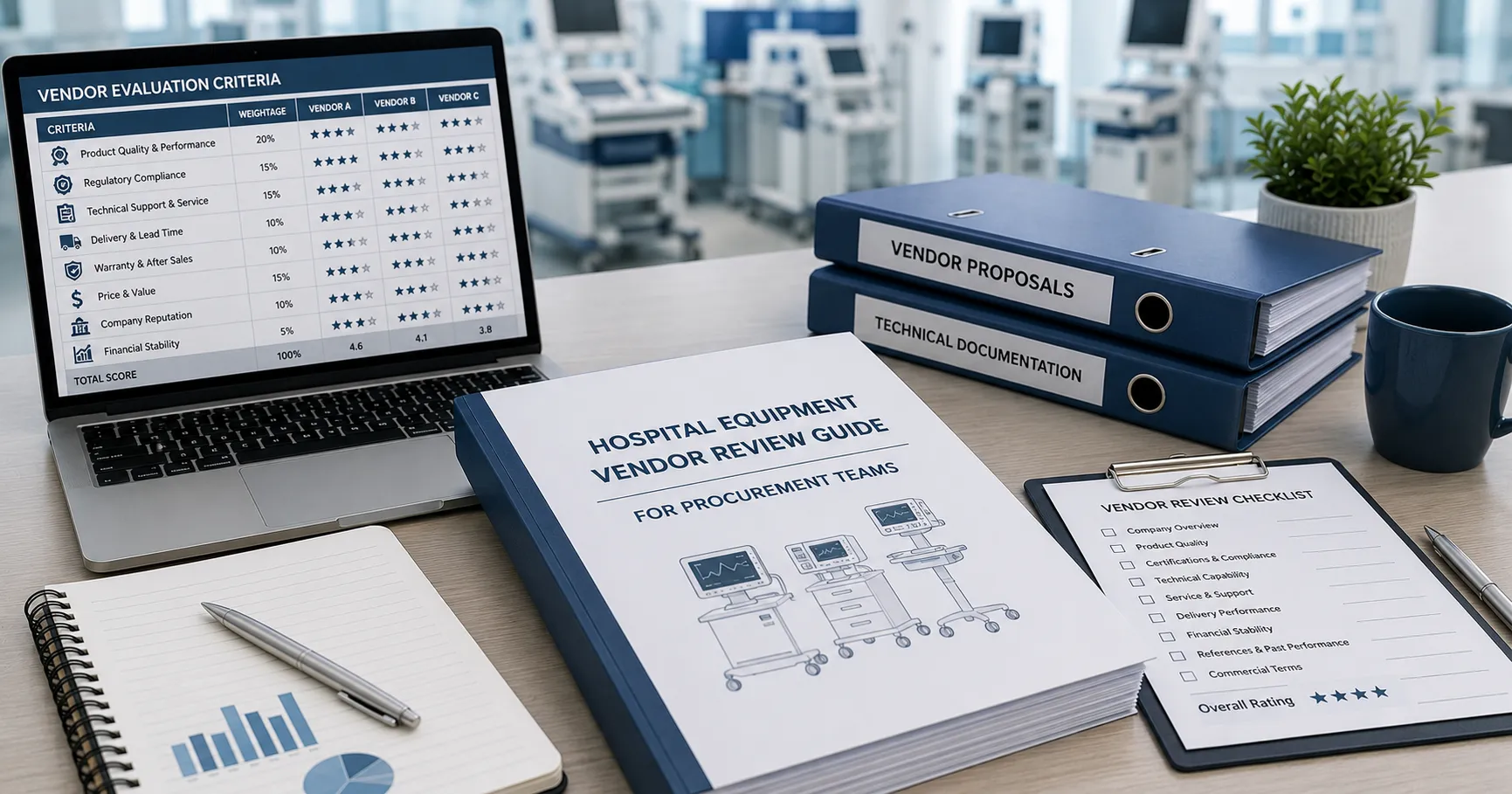
This guide explains how hospital buyers can assess equipment service response, compare support arrangements and build measurable requirements into procurement decisions.
Why Service Response Directly Affects Clinical Operations
Service response refers to the complete process that begins when a healthcare facility reports an equipment problem. It includes acknowledgement, fault assessment, technical escalation, engineer attendance, parts supply, repair and return to clinical use.
Clinical criticality determines urgency — The acceptable response for an examination couch will differ from the response required for a ventilator, defibrillator or laboratory analyser. Buyers should classify equipment according to the consequences of failure and the availability of backup capacity.
In practice, procurement teams often find that suppliers offer a single standard response target across all product categories. This may be unsuitable where clinical risk differs considerably.
Acknowledgement is not resolution — A supplier may respond quickly to an email without taking meaningful action. Service requirements should distinguish initial acknowledgement, technical diagnosis, engineer attendance and completed repair.
Each stage should have a measurable target.
Downtime creates wider costs — Repair expenditure represents only part of the financial impact. Equipment failure can cause cancelled appointments, patient transfers, staff disruption, delayed reporting and additional rental expenditure.
These operational costs should be considered when comparing service packages.
Local technical capacity matters — Facilities with biomedical engineering teams may resolve minor faults internally. Other sites depend entirely on external service providers and require faster access to trained engineers.
The supplier should understand which activities the hospital can perform and which require authorised technical support.
Communication supports clinical planning — Clinical departments need realistic updates when equipment cannot be restored immediately. A useful service provider gives clear fault status, parts availability and expected restoration information rather than repeated general assurances.
Service response should therefore be assessed as part of clinical continuity planning, not treated solely as a maintenance issue.
Service Expectations Across Different Healthcare Settings
Equipment support requirements vary with facility size, location, workload, and available technical resources.
Large hospitals and teaching facilities — Major hospitals may maintain internal engineering teams, workshops and spare-parts inventories. External suppliers may provide specialist diagnostics, software access, major repairs and manufacturer escalation.
These facilities often require service records to integrate with central asset-management systems.
District and regional hospitals — Regional facilities may have fewer engineering resources and longer travel distances from service centres. Buyers working with trusted international healthcare supplier
partners should confirm whether stated response times apply to the hospital’s actual location.
Experienced clinical supply managers typically request evidence of previous engineer attendance in comparable locations rather than relying on regional coverage maps.
Community clinics and outpatient centres — Smaller facilities may not require continuous on-site support, but they still need clear escalation contacts and dependable replacement arrangements. Portable loan equipment can sometimes provide better continuity than an expensive rapid-attendance contract.
Diagnostic and laboratory facilities — analyser, imaging, and diagnostic system failures can interrupt high-volume services. Remote diagnostics, application support and access to calibrated replacement components may be essential.
Reagent and software compatibility should also form part of the support review.
Mobile and remote healthcare services — Physical engineer attendance may be difficult in mobile or isolated settings. Service plans should emphasise remote troubleshooting, modular replacement, operator guidance and pre-positioned spare parts.
Multi-facility healthcare networks — Groups managing several sites may use central service contracts with different response levels by location. Buyers should ensure that every facility understands how to report faults and escalate unresolved cases.
Service expectations should reflect the actual operating environment rather than the supplier’s standard package alone.
Technical Service Terms Buyers Should Examine
Service proposals often use similar language while providing very different levels of support. Buyers should define each requirement in measurable terms.
Response-time definitions — The contract should specify when the response clock begins and what constitutes a response. An automated acknowledgement should not be treated as a technical diagnosis unless that is explicitly agreed upon.
Targets may be measured in working hours, calendar hours or business days, so the wording must remain clear.
Engineer availability — Buyers should ask where engineers are based, which products they are trained to service and how holiday or absence cover is managed. Claimed coverage has limited value when only one qualified engineer supports a large region.
Remote diagnostic capability — Connected equipment may allow technicians to review error logs, software status and system performance remotely. This can reduce diagnostic time, but access must be secured through authorisation and comply with applicable data-protection requirements.
Spare parts access — Service response depends heavily on whether the required parts are stocked locally or ordered internationally. Suppliers should provide typical lead times, stock arrangements, and information on parts support throughout the expected equipment life.
First-time repair capability — Fast attendance does not guarantee rapid restoration. Engineer competence, diagnostic tools and access to likely replacement parts affect whether the fault can be resolved during the first visit.
Loan and replacement equipment — Hospitals should confirm whether temporary replacement equipment is available, how quickly it can be delivered and who pays for transportation or installation. Loan equipment must remain clinically suitable and supported by appropriate documentation.
Service reporting — Reports should record the reported fault, diagnostic findings, work completed, parts fitted, safety checks and restoration status. Incomplete reports weaken maintenance history and future replacement decisions.
Technical service terms should allow procurement teams to compare measurable support rather than broad promises of rapid assistance.
Comparing Service Providers During Procurement
Service evaluation should take place alongside technical and commercial assessment. Negotiating support only after equipment selection weakens the buyer’s ability to compare alternatives.
Calculate the supported ownership cost — Buyers should combine the equipment price with preventive maintenance, corrective repairs, software, engineer travel, spare parts,s and potential downtime. A higher purchase price may offer better value when dependable support is included.
Request a detailed service schedule — Bidders should separate warranty support, preventive maintenance and chargeable repair services. Labour, travel, freight, software and parts exclusions should be stated clearly.
Evaluate published support claims — Healthcare equipment vendors advertising across global markets should present accurate service coverage, warranty information and regional support capability. Procurement teams should verify these statements against written contract terms and operational evidence.
Check technical competence — Supplier experience should relate to the exact product family being offered. Buyers may request engineer training records, service references, diagnostic capability and escalation access to the manufacturer.
Define performance measures — Contracts may monitor acknowledgement time, attendance time, repair duration, first-time resolution, and repeat failures. Each measure should have a clear calculation method and reporting frequency.
Review escalation arrangements — Buyers should know who becomes responsible when the initial support contact cannot resolve the fault. Escalation routes should include technical, operational and commercial contacts.
Healthcare networks making repeated purchases may obtain more consistent support through long-term medical equipment supply partnerships. These arrangements should define service coverage by location, performance expectations and consequences for repeated failures.
Maintaining Service Quality Throughout Equipment Life
Service capability can decline as equipment ages, engineers leave, or manufacturers discontinue components. Buyers should monitor support throughout the full ownership period.
Preventive maintenance performance — Scheduled servicing should occur at the agreed intervals and follow manufacturer recommendations. Missed visits, incomplete checks and unsigned reports should be investigated.
Preventive maintenance records can also identify recurring wear and future parts requirements.
Corrective repair history — Procurement and engineering teams should track the frequency, severity and duration of breakdowns. Repeated faults may indicate unsuitable operation, unresolved technical problems or declining equipment reliability.
Spare-parts continuity — Suppliers should provide early notice when key components approach discontinuation. Hospitals may need to purchase strategic spares, identify alternative support or bring forward replacement planning.
Software and cybersecurity support — Connected equipment may require security updates, licence renewal and compatibility management. Buyers should confirm how long software support will remain available and how vulnerabilities are communicated.
Operator training — Some reported faults result from incorrect setup, cleaning or accessory use. Refresher training and clear user guidance can reduce avoidable service requests.
Performance review meetings — Regular reviews should compare actual response performance with agreed targets. Persistent delays require corrective action, revised support arrangements or alternative service planning.
In markets with limited local technical coverage, international travel and prolonged parts delivery can cost more than the repair itself. Service-life planning should therefore include support availability, not only equipment age and condition.
International Support, Logistics and Escalation Risk
International equipment purchasing introduces additional service risks because the seller, manufacturer, engineer and parts warehouse may operate in different locations.
Cross-border warranty terms — Buyers should verify whether warranty coverage remains valid in the destination market. Engineer travel, accommodation, parts freight, customs and local labour may not be included.
Parts import requirements — Replacement components may require export paperwork, customs clearance or regulatory documentation. These processes can extend downtime even when the part is immediately available at the supplier’s warehouse. Time zone and communication controls — International support teams may not operate during the hospital’s working hours. Buyers should confirm emergency contacts, service hours and escalation arrangements.
Remote-support security — Remote access should use controlled credentials, documented authorisation and secure technical processes. Healthcare facilities should also determine who may approve external access to connected equipment.
Local service partnerships — A supplier may rely on regional engineers or independent service organisations. Buyers should verify training, responsibilities, access to parts and the process for managing service quality.
Procurement support — Hospital buyers assessing international equipment, warranties or regional service arrangements can contact Medigear.uk for international supply enquiries. A useful enquiry should include the equipment type, destination, quantity, required response level and expected support period.
International service plans work best when every responsibility is confirmed before shipment rather than after the first breakdown.
Final thoughts
Medical equipment service response should be evaluated as carefully as clinical performance and purchase price. A device that cannot be repaired promptly may create operational disruption, unplanned expenditure and avoidable pressure on patient services.
Hospital buyers should define acknowledgement, diagnostic, attendance and repair targets separately. They should also verify engineer capability, parts access, remote support, warranty exclusions and escalation arrangements.
Disclaimer
Medigear.uk is a global medical equipment supplier, exporter, and distributor. The content published on this site is intended for educational and product awareness purposes only. Nothing on this page constitutes medical advice, clinical guidance, or treatment recommendations. All healthcare procurement and clinical decisions should be made by qualified medical professionals and compliant procurement teams operating within the regulatory frameworks of their respective countries.