Alfie Cooper
Alfie Cooper Hospital equipment rarely fails according to a convenient capital schedule. A device may remain operational while repair costs rise, software support ends, or clinical demand exceeds its original capacity. Another asset may appear old but continue to perform safely with dependable maintenance and spare parts readily available.
For healthcare buyers, hospital equipment replacement planning creates a structured method for deciding which assets should be renewed, when procurement should begin and how limited capital should be prioritised. Replacement decisions should not depend only on equipment age or a single breakdown.
Medical managers need evidence covering clinical risk, condition, utilisation, maintenance history, technology support and total cost of ownership. They must also coordinate replacement with infrastructure readiness, staff training and service continuity.
A controlled plan reduces emergency purchases and helps facilities avoid retaining equipment that has become unreliable, unsupported or unsuitable. This guide explains how medical managers can assess replacement needs, rank assets, and manage the transition to new or professionally refurbished equipment.
What Replacement Planning Controls in Clinical Operations
Equipment replacement planning connects asset management with clinical service delivery. Its purpose is to identify declining assets before their condition causes avoidable disruption, safety concerns or uncontrolled expenditure.
Clinical risk exposure — Medical managers should assess what happens if a device becomes unavailable or performs incorrectly. Life-support, emergency, diagnostic and infection-control equipment generally require closer monitoring because failure may have immediate consequences.
In practice, procurement teams often find that the highest-cost assets are not always the most urgent replacements. Lower-value equipment can carry a significant risk when no backup is available.
Service continuity requirements — Replacement decisions should consider whether the facility has alternative equipment, shared capacity or access to external services. A device may require earlier replacement where failure would stop an entire clinical pathway.
Where backups exist, the facility may have more time to plan procurement and installation.
Current clinical suitability — Equipment may still function but no longer support the facility’s workload, patient population or clinical practice. Limited throughput, unsuitable accessories or weak connectivity can reduce operational value.
Reliability and downtime — Repeated breakdowns can disrupt appointments, procedures and staff schedules. Managers should track fault frequency, repair duration and recurrence rather than considering each service incident separately.
Supportability — Equipment becomes difficult to retain when spare parts, software updates, consumables or qualified engineers are no longer available. A functioning device can therefore reach the end of its practical service life before complete mechanical failure.
Financial predictability — Planned replacement allows capital, installation and training costs to be forecast. Emergency purchases often reduce buyer choice and weaken the facility’s ability to compare configurations, suppliers and support terms.
A useful replacement plan, therefore, protects clinical capacity while giving finance and procurement teams enough time to make evidence-based decisions.
How Replacement Priorities Vary Across Healthcare Settings
Replacement criteria should reflect the facility’s clinical role, technical resources and access to alternative equipment. A single age-based rule is unlikely to work across every healthcare environment.
Large hospitals and teaching facilities — Major hospitals may manage thousands of devices across imaging, critical care, surgery, laboratory and general wards. Replacement programmes often require multi-year capital planning, departmental prioritisation and coordination with construction or digital-system projects.
These facilities should also assess whether standardisation across departments could reduce training, accessory and maintenance costs.
District and regional hospitals — Regional facilities may depend on fewer units and have limited technical support. When obtaining replacement options from specialist medical equipment supplier networks, managers should verify delivery times, installation capability, spare parts access and support at the actual facility location.
Experienced clinical supply managers typically assign greater urgency to equipment that lacks a local repair pathway, even when its current condition appears acceptable.
Community clinics and outpatient centres — Smaller facilities may have restricted capital and little backup capacity. Replacement decisions should favour dependable equipment with manageable infrastructure, training and maintenance requirements.
Premium functions that will rarely be used may provide less value than a simpler, well-supported configuration.
Diagnostic centres and laboratories — Diagnostic systems may become obsolete because reagents, software, quality controls or interfaces are discontinued. Replacement planning should therefore assess the complete operating platform rather than only the main analyser or imaging unit.
Mobile and remote healthcare services — Portable equipment experiences transport, charging and environmental stress. Batteries, protective housings and connectors may deteriorate more quickly than they would in a fixed clinical setting.
Multi-facility healthcare groups — Central planning can identify shared demand, bulk-purchasing opportunities, and transferable equipment. However, each site’s workload, infrastructure and support access should remain visible in the final priority ranking.
Replacement programmes are stronger when they reflect actual clinical conditions instead of applying one universal service-life assumption.
Asset Data and Technical Criteria That Trigger Replacement
Medical managers need reliable asset information before deciding whether equipment should be repaired, upgraded or replaced. Incomplete inventories can lead to both premature disposal and prolonged use of unsuitable devices.
Verified asset identity — Records should include manufacturer, model, serial number, location, installation date and ownership status. Managers should also identify accessories, software versions and linked systems that may be affected by replacement.
Condition and safety history — Inspection results, calibration failures, recalls, safety notices and recurring defects should form part of the assessment. A device with repeated safety-related issues may require urgent action even where repairs remain technically possible.
Maintenance cost trend — Annual repair expenditure should be reviewed over several periods. Rising cost, frequent engineer visits and repeated component failure may show that continued maintenance is no longer financially sustainable.
The decision should consider both the direct repair cost and the disruption caused by downtime.
Utilisation and capacity — Equipment that is heavily used may reach its practical service limit earlier than a lightly used asset of the same age. Managers should assess operating hours, procedure volume, test throughput and peak demand.
Parts and software availability — Manufacturer support status can influence replacement timing. Equipment may require renewal when critical components, operating software or cybersecurity updates are no longer available.
Compatibility with current systems — Older devices may not integrate with hospital networks, imaging archives, laboratory systems or electronic records. Workarounds can create inefficiency, cybersecurity exposure and transcription errors.
Energy and resource consumption — Newer equipment may reduce electricity, water, gases or consumable waste. These savings should be measured realistically and balanced against acquisition and implementation expenditure.
Expected remaining service life — A replacement decision should estimate how long the equipment can remain safe, reliable and supportable. This is more useful than applying a fixed age limit without considering the actual condition.
Technical criteria should explain why replacement is required and what operational improvement the new equipment must deliver.
How Medical Managers Should Approve Replacement Decisions
Replacement approval should use consistent criteria across departments. Without a structured method, high-profile requests may receive funding while less visible clinical risks remain unresolved.
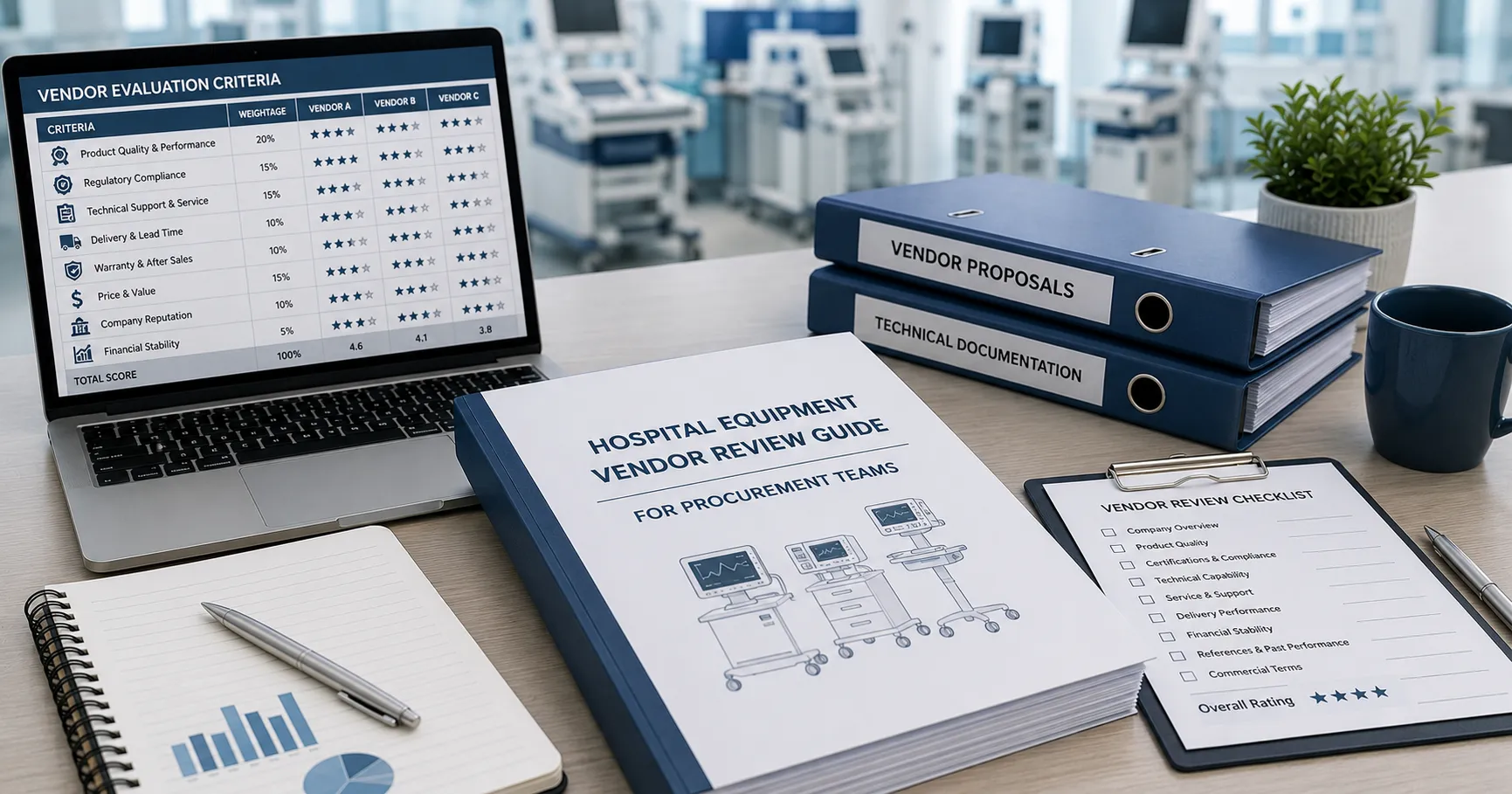
Create a weighted priority score — Medical managers can score clinical risk, condition, downtime, utilisation, maintenance cost and support status. Weightings should reflect organisational priorities and equipment criticality.
Mandatory replacement triggers, such as unresolved safety concerns, should remain separate from general scoring.
Compare repair, upgrade and replacement options — Replacement is not always the only suitable response. Software updates, component replacement, refurbishment or redeployment may extend useful life where clinical and compliance requirements remain satisfied.
Assess total implementation cost — The budget should include equipment, accessories, freight, installation, room modifications, integration, training, service and disposal. The headline product price alone does not reflect the full financial commitment.
Review supplier information carefully — Equipment manufacturers advertising to global hospital buyers should provide clear specifications, configuration details, compliance documentation and support terms. Managers should compare these claims with formal quotations and technical evidence.
Plan service continuity — Replacement may require equipment shutdown, removal, construction work and staff training. The project plan should identify temporary capacity, phased installation, or loan equipment requirements.
Verify regulatory suitability — Replacement equipment should meet applicable local regulatory standards, including standards such as CE, FDA or regional equivalents where relevant. Destination-specific registration and import requirements should be confirmed before ordering.
Medical managers responsible for recurring replacement programmes may benefit from formal international supply chain partnerships. These arrangements should still include competitive review, measurable service standards and clear accountability for delivery, installation and support.
Using Maintenance History to Estimate Remaining Service Life
Maintenance data helps distinguish equipment that is old but dependable from equipment that is becoming costly or unsafe to retain. Service history should therefore influence both timing and priority.
Preventive maintenance compliance — Managers should verify that recommended inspections and calibrations were completed on schedule. A poor maintenance history may shorten the remaining service life or make condition assessment less reliable.
Breakdown frequency — A rising number of faults can signal component wear, environmental stress or declining parts quality. Repeated failures of the same component require investigation rather than separate repair decisions.
Repair duration — Long downtime may result from limited engineer access or international parts supply. Even infrequent failures can justify replacement when each incident takes essential equipment out of service for an extended period.
Cost of continued ownership — Maintenance contracts, call-out charges, parts, software and backup arrangements should be included. Facilities in markets with limited local service often find that travel and freight costs exceed the value of the component being replaced.
Support withdrawal dates — Manufacturers and service providers may announce the end of software, parts or technical support. These dates should feed directly into capital planning rather than being addressed after support has ended.
Maintenance-related clinical disruption — Managers should document cancelled procedures, delayed tests and equipment transfers caused by faults. This evidence gives decision-makers a clearer view of the operational cost of retaining the asset.
Replacement does not always eliminate maintenance expenditure. New equipment may require service contracts, software licences and specialised training, so projected ownership costs should be compared on the same basis.
International Sourcing and Replacement Project Delivery
Replacing hospital equipment through international sourcing can improve access to suitable products, but it adds logistical, regulatory and service considerations.
Lead-time planning — Manufacturing, refurbishment, export preparation, transport, customs clearance and installation should be scheduled separately. Procurement should begin before the existing asset reaches an unacceptable level of risk.
Delivery and import costs — Budgets should identify freight, insurance, customs, taxes, inspection, storage and local transport. Responsibilities should be clear under the agreed commercial terms.
New and refurbished options — New equipment may provide longer support life and stronger warranty coverage. Professionally refurbished equipment can reduce capital expenditure where condition, service history, compliance, software and parts availability are verified.
Infrastructure readiness — Replacement models may have different power, network, ventilation, water, gas or space requirements. Site assessments should be completed before shipment.
Training and commissioning — The plan should identify operator training, technical instruction, acceptance testing and documentation requirements. Equipment should not enter routine use until implementation responsibilities have been completed.
Specialist replacement support — Medical managers planning international purchases or multi-category renewal programmes can contact the Medigear.uk team for supply support. A detailed enquiry should include equipment categories, quantities, destinations, condition preferences, and planned delivery schedules.
International sourcing should be coordinated with the removal of the existing asset. Storage, data removal, decontamination, resale, recycling and compliant disposal responsibilities must be confirmed before installation begins.
Final thoughts
Hospital equipment replacement planning helps medical managers move from reactive purchasing to controlled asset renewal. Equipment age can inform the decision, but it should not act as the only replacement trigger.
Clinical risk, reliability, utilisation, maintenance cost, support availability and technology compatibility provide stronger evidence. These factors should be scored consistently and supported by asset, service and financial records.
Disclaimer
Medigear.uk is a global medical equipment supplier, exporter, and distributor. The content published on this site is intended for educational and product awareness purposes only. Nothing on this page constitutes medical advice, clinical guidance, or treatment recommendations. All healthcare procurement and clinical decisions should be made by qualified medical professionals and compliant procurement teams operating within the regulatory frameworks of their respective countries.